.webp)

Chest pain creates immediate concern. You often think of the heart or lungs first. In many patients, diagnostic tests show no cardiac or pulmonary disease. A frequent but underrecognized cause is nerve pain. Intercostal neuralgia is a neuropathic pain condition involving the nerves between the ribs. It produces sharp, burning, or electric pain that often worsens with breathing or movement. Identifying nerve involvement early helps reduce fear and guides effective treatment.
Next, you will read what intercostal neuralgia is and how rib nerves generate pain.
Intercostal neuralgia is pain caused by irritation, compression, or injury of the intercostal nerves. These nerves exit the thoracic spine and travel along each rib toward the chest wall and upper abdomen. When nerve signaling becomes abnormal, pain continues even after tissues heal. This explains why rib pain can persist for months after surgery, infection, or trauma.
The next section explains what commonly damages or irritates these nerves.
Thoracic surgery stretches or scars intercostal nerves. Lung surgery, mastectomy, cardiac surgery, and chest tube placement are frequent triggers. Studies report chronic post thoracotomy pain in up to 50 percent of patients.
Rib fractures, falls, sports injuries, and repetitive twisting strain the intercostal nerves. Even minor trauma can cause prolonged nerve sensitivity.
Herpes zoster, also called shingles, inflames sensory nerves. Postherpetic neuralgia develops in about 10 to 20 percent of shingles cases, especially in adults over 60.
Thoracic disc degeneration, arthritis, or spinal stenosis compress nerve roots. Compression alters nerve conduction and produces radiating rib pain.
Next, you will see how patients typically describe their symptoms.
Intercostal neuralgia produces consistent symptom patterns:
Symptoms may be constant or episodic. Intensity often fluctuates during the day. The following section explains why this condition is often missed.
Chest pain triggers appropriate emergency evaluation. Cardiac and pulmonary causes must be excluded first. Once tests return normal, patients are sometimes told the pain is muscular or stress related. Nerve pain lacks visible imaging findings. Without a focused neurologic exam, intercostal neuralgia may remain undiagnosed. Delayed recognition increases anxiety and prolongs suffering.
Next, you will learn about evidence based treatment options.
Treatment targets abnormal nerve signaling, mechanical irritation, and pain related fear.
Neuropathic agents such as gabapentin, pregabalin, or tricyclic antidepressants reduce nerve firing. Clinical trials show partial relief in many patients, but sedation and dizziness are common side effects.
Therapy improves thoracic mobility and posture. Targeted exercises reduce rib joint stiffness and nerve tension. Manual therapy may help when pain has a mechanical component.
Local anesthetic or steroid injections around the intercostal nerve provide diagnostic and temporary relief. Duration ranges from days to weeks. Repeated injections carry procedural risks.
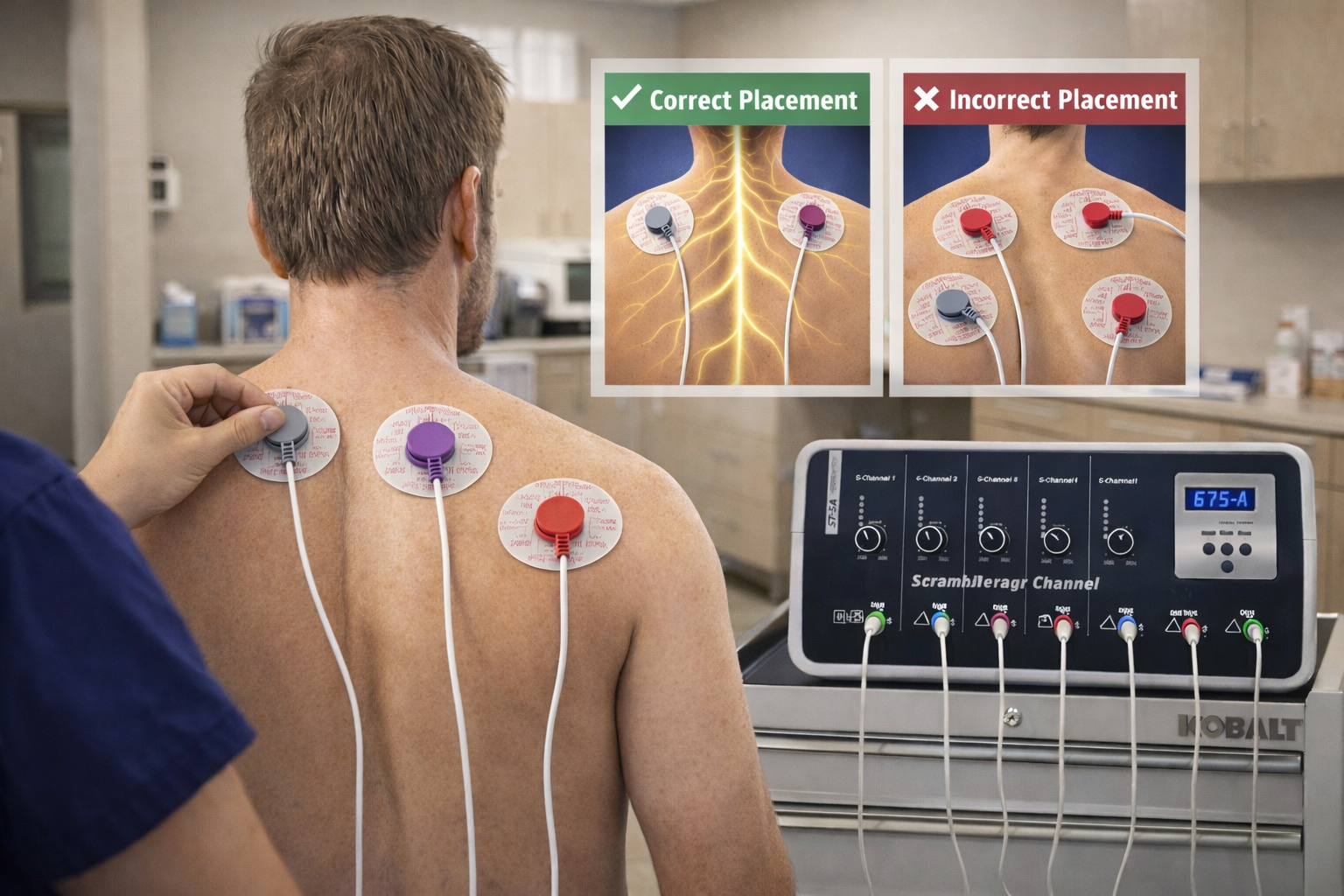
Scrambler Therapy uses surface electrodes to replace pain signals with non pain information. Clinical studies show significant pain reduction in chronic neuropathic conditions without injections or surgery.
Next, you will read what patients commonly experience in a clinical setting.
Most patients arrive fearing serious disease. Once nerve pain is identified, understanding the diagnosis often reduces symptom severity. Education lowers stress, improves adherence, and enhances treatment response. Patients with earlier intervention report better functional recovery.
The next section explains when urgent evaluation is still required.
You should seek immediate care if chest pain occurs with:
After life threatening causes are excluded, evaluation for intercostal neuralgia becomes appropriate. Early referral improves outcomes. Below are frequently asked questions patients raise.
It feels burning, stabbing, or electric along the ribs and chest wall.
It is usually not life threatening but requires evaluation to exclude serious causes.
Yes. Some cases resolve spontaneously. Others need structured treatment.
Physical therapy and neuromodulation such as Scrambler Therapy are non-invasive options.
Yes. Poor posture increases thoracic nerve compression and symptom severity.
This content is for educational purposes only. It does not replace medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for persistent or severe symptoms.

Discover South Florida Scrambler Therapy is one of the nation’s leading clinics for noninvasive chronic pain relief, offering FDA-cleared Scrambler Therapy® for adults and children. Co-founded by Dr. Rick Markson, one of the few practitioners worldwide to receive advanced certification directly from the therapy’s inventor in Rome, our clinic delivers globally recognized expertise with compassionate, personalized care. If you or a loved one is living with treatment-resistant nerve pain, we invite you to schedule a consultation and explore a life beyond pain.
Scrambler Therapy FDA FDA 510(k) database
Scrambler Therapy delivers 80%–90% pain reduction for patients suffering from nerve-related pain.
Pain Physician Journal study on Scrambler Therapy’s effectiveness
Scrambler therapy is a non-invasive, opioid-sparing treatment for chronic pain.
📘 What is scrambler therapy?
📘 What to Expect During a Scrambler Session
📘 CRPS Pain Relief Without Drugs—Real Patient Stories
📘 Conditions that scrambler therapy can treat
Keep up to date with important news about our clinic and your medical records.